Does SVT have P waves
 John Peck
John Peck Sinus tach and most SVTs have only one P wave for each QRS complex. They may or may not be buried in the preceding T waves. But there are other supra-ventricular tachycardias that have more than one P wave for each QRS or no P waves. Atrial fibrillation has no P waves.
Can you see P waves in SVT?
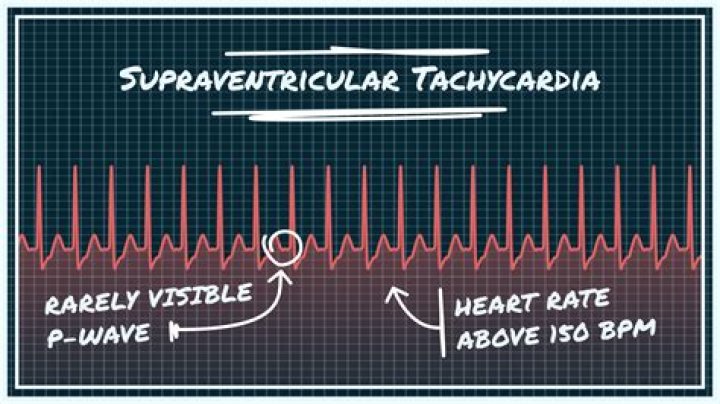
In SVTs with rapid ventricular rates, P waves are often obscured by the T waves, but may be seen as a “hump” on the T. A heart rate of 150 should make you suspect atrial flutter is present.
Is QRS normal in SVT?
Supraventricular tachycardia (SVT) is a dysrhythmia originating at or above the atrioventricular (AV) node and is defined by a narrow complex (QRS < 120 milliseconds) at a rate > 100 beats per minute (bpm).
What does SVT look like on ECG?
Supraventricular tachycardias are usually narrow-complex tachycardias with a QRS interval of 100 ms or less on an electrocardiogram (ECG). Occasionally, they may show a wide QRS complex in the case of a pre-existing conduction delay, an aberrancy due to rate-related conduction delay or a bundle branch block.What's the difference between SVT and Vtach?
Tachycardia can be categorized by the location from which it originates in the heart. Two types of tachycardia we commonly treat are: Supraventricular tachycardia (SVT) begins in the upper portion of the heart, usually the atria. Ventricular tachycardia (VT) begins in the heart’s lower chambers, the ventricles.
How do you know if you have supraventricular tachycardia?
- Very fast (rapid) heartbeat.
- A fluttering or pounding in your chest (palpitations)
- A pounding sensation in the neck.
- Weakness or feeling very tired (fatigue)
- Chest pain.
- Shortness of breath.
- Lightheadedness or dizziness.
- Sweating.
When do you Cardiovert SVT?
Unstable patients with SVT and a pulse are always treated with synchronized cardioversion. The appropriate voltage for cardioverting SVT is 50-100 J. This is what AHA recommends and also SVT converts quite readily with 50-100 J.
How can you tell the difference between SVT and atrial flutter?
This is because the P waves (flutter waves) in atrial flutter occur at about 250-350 per minute (usually around 300). At this rate, it can appear that there is a P wave in front of each QRS and a T wave after each QRS. This causes the misdiagnosis of sinus tachycardia or SVT.How is the diagnosis of SVT determined?
How is SVT diagnosed? Your doctor will diagnose SVT by asking you questions about your health and symptoms, doing a physical exam, and perhaps giving you tests. Your doctor: Will ask if anything triggers the fast heart rate, how long it lasts, if it starts and stops suddenly, and if the beats are regular or irregular.
Do you Anticoagulate for SVT?Synchronized cardioversion is recommended (moderate-quality evidence) for the termination of any hemodynamically unstable SVT. In the absence of hemodynamic compromise, SVT should be treated (moderate-quality evidence) with synchronized cardioversion when pharmacologic therapy is ineffective or contraindicated.
Article first time published onHow are P waves different from T waves?
‘P’ wave is the first wave in an ECG and is a positive wave. It indicates the activation of the SA nodes. ‘T’ wave too is a positive wave and is the final wave in an ECG though sometimes an additional U wave may be seen. It represents ventricular relaxation.
Does SVT require anticoagulation?
As it currently stands, a detailed discussion of anticoagulation is omitted from the SVT guideline, which simply references the AF guideline, requiring the reader to search out another document for specific recommendations.
Can you have both SVT and VT?
The short answer is yes, but it can be very difficult, and even experienced clinicians can misdiagnose VT as SVT with aberrancy! This can lead to clinical misadventure.
Is SVT shockable?
The shock that is delivered for SVT is synchronized to occur at a precise time during the “R” wave on the EKG, so as to avoid the vulnerable refractory period which could cause ventricular fibrillation.
What rhythms do you Cardiovert?
An electrical cardioversion, often referred to simply as a cardioversion, is a procedure used to treat an abnormal and rapid heart rhythm (also called a cardiac arrhythmia). The most commonly treated arrhythmia is atrial fibrillation. Another rhythm commonly treated with electrical cardioversion is atrial flutter.
What is vagal maneuvers for SVT?
Vagal maneuvers are used to try to slow an episode of supraventricular tachycardia (SVT). These simple maneuvers stimulate the vagus nerve, sometimes resulting in slowed conduction of electrical impulses through the atrioventricular (AV) node of the heart.
What causes SVT to develop?
SVT is usually a result of faulty electrical signaling in your heart. It’s commonly brought on by premature beats. Some types of SVT run in families, so genes may play a role. Other types may be caused by lung problems.
Is AFIB with RVR considered SVT?
Atrial fibrillation and atrial flutter are both types of SVT that are more common in older patients or patients with preexisting heart conditions. Atrial fibrillation can be more serious because, for some patients, it can lead to blood clots and increase stroke risk.
Do I have SVT or AFIB?
In terms of differences, atrial fibrillation may cause blood clots to form and produce weakness, whereas SVT may cause chest pain, fainting and tightening of the throat. Atrial fibrillation causes the atria to not fully contract, whereas in SVT, the atria contract excessively fast.
Is atrial flutter a supraventricular tachycardia?
Atrial fibrillation and atrial flutter The heart’s upper chambers (atria) beat irregularly. But it is not commonly considered a type of SVT. Atrial flutter is like atrial fibrillation, because the electrical problem is in the atria. But with atrial flutter, the heart beats very fast in a regular rhythm.
What is SVT Google Scholar?
Supraventricular tachycardia (SVT) is a heterogeneous group of arrhythmias used to describe tachycardias that involve cardiac tissue at the level of the bundle of His or above. 1. The prevalence of SVT is 2.25/1000 persons with a female predominance of 2:1 across all age groups.
What do you do for ACLS SVT?
- Attempt vagal maneuvers.
- If unsuccessful, administer adenosine 6 mg IV bolus followed by a rapid normal saline flush.
- If unsuccessful, administer adenosine 12 mg IV bolus followed by a rapid normal saline flush.
What rate is SVT?
A normal resting heart rate is usually between 60 and 100 beats a minute. Anything over 100 is considered tachycardia. SVT rates are usually about 150 to 250 beats a minute.
What is the P wave do?
The P wave represents the electrical depolarization of the atria. In a healthy person, this originates at the sinoatrial node (SA node) and disperses into both left and right atria.
What do P QRS and T waves represent?
The P wave in an ECG complex indicates atrial depolarization. The QRS is responsible for ventricular depolarization and the T wave is ventricular repolarization.
How do you find the P wave on an ECG?
The P wave represents depolarization of the right and left atria. Onset of the P Wave is identified as: the first abrupt or gradual deviation from the baseline. The point where the wave returns to the baseline marks the end of the P Wave. A QRS complex normally follows each P Wave.
Can you shock pulseless SVT?
Shockable Rhythm: Pulseless V-tach Ventricular tachycardia (V-tach) will usually respond well to defibrillation.
Will an AED shock SVT?
For VT and SVT, it also verified that the ratios of the shock advice differed for each AED. The accuracy of the ECG rhythm analysis was elucidated for each AED. This study revealed that AEDs could advise to deliver shocks for SVTs, especially those with a wide QRS complex.
Why is asystole not shockable?
Pulseless electrical activity and asystole or flatlining (3 and 4), in contrast, are non-shockable, so they don’t respond to defibrillation. These rhythms indicate that the heart muscle itself is dysfunctional; it has stopped listening to the orders to contract.